Many parents first notice daytime mouth breathing when they look at photos of their child or watch them quietly concentrating on a screen. The lips are apart, the jaw is slightly dropped and the air clearly seems to be moving in through the mouth rather than the nose. At first this can look harmless or simply part of how a child holds their face, especially if it has been that way for a long time.
Short periods of mouth breathing are common with colds and flu and usually settle as the nose clears. When daytime mouth breathing persists for months and is combined with snoring or disturbed sleep, it can sometimes be a sign that the airway is not working as well as it should. For some children it is linked with nasal blockage, enlarged adenoids and tonsils, allergies or obstructive sleep apnoea.
At Melbourne ENT in St Kilda East, Victoria, ENT and Head & Neck Surgeon Dr Simon Braham regularly assesses children who have been referred because of ongoing mouth breathing, noisy breathing, snoring or concerns about sleep and daytime behaviour. This article explains what daytime mouth breathing is, when it may be a sign of an airway problem, what an ENT assessment involves and how treatment decisions are made. It is general information for families in Melbourne and surrounding areas and does not replace personal medical advice.
What is daytime mouth breathing in children?
✓ How children normally breathe
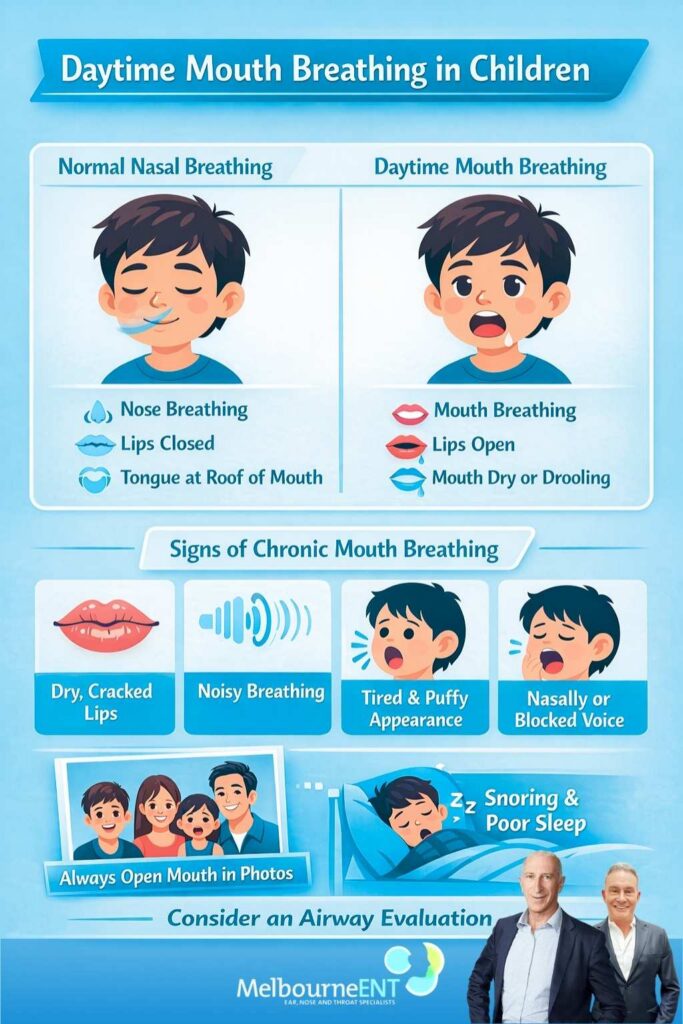
In healthy children, quiet breathing at rest usually occurs through the nose. The nose filters dust and particles, warms and moistens the air and delivers it efficiently into the lungs. When nasal breathing is easy, the lips can stay gently closed, the tongue rests against the roof of the mouth and the jaw and facial muscles can relax. This pattern supports comfortable, quiet breathing and normal facial and dental development.
✓ What we mean by “daytime mouth breathing“
Daytime mouth breathing refers to a pattern where a child habitually keeps the lips parted and draws most of their air in through the mouth while awake. Parents may notice it when the child is playing quietly, reading, watching television, sitting in the car or listening in class. It is different from occasional mouth breathing during vigorous exercise or during a short lived cold.
The key point is that mouth breathing has become the default, even when the child is relaxed and does not appear unwell. The nose may not be completely blocked, but nasal breathing does not seem easy or natural and the child looks more comfortable breathing through the mouth.
✓ Signs that mouth breathing has become your child’s “new normal“
When mouth breathing becomes a long term pattern there are often other hints. Some children have dry or cracked lips because the mouth is open at rest. Others dribble slightly or have a constantly damp chin. Their voice can sound blocked or nasal, as if they always have a mild cold. Teachers or carers may comment that the child breathes noisily even when sitting quietly, or that they often look “puffed” without obvious exertion.
Parents sometimes notice that in family photographs their child is frequently the only one with an open mouth while everyone else has relaxed closed lips. If this pattern has been present for many months, and especially if there is also snoring or poor sleep, it is reasonable to think about possible airway problems rather than assuming it is just a habit.
Is daytime mouth breathing always a sign of airway problems?
✓ Short term versus ongoing symptoms
Not all mouth breathing is a sign of serious disease. During colds and upper respiratory infections the nose can be blocked for a week or two. During this time children often switch naturally to breathing through the mouth and then return to normal nasal breathing once the infection settles. Short lived episodes like this are very common.
Concerns arise when mouth breathing persists long after a cold has cleared or keeps returning throughout the year without a period of comfortable nasal breathing in between. If a child who appears otherwise well continues to breathe through their mouth most days for several months, this is more in keeping with an ongoing problem that should be properly assessed.
✓ Red flags that suggest the airway might be narrowed
Daytime mouth breathing becomes more significant when it occurs together with other features. Parents might notice regular snoring at night rather than only when their child is unwell. They may see pauses in breathing, gasping or very heavy breathing during sleep. Some children toss and turn, sweat, wake repeatedly or adopt unusual positions such as arching the neck to keep the airway open. During the day they can be irritable, flat, overly energetic or seem to drift off in class.
When mouth breathing forms part of this wider picture, it can indicate that the airway is narrowed at the level of the nose, adenoids and tonsils or throat. In these situations GPs and paediatricians in Melbourne often refer families to an ENT specialist such as Dr Simon Braham at Melbourne ENT to consider whether sleep disordered breathing or obstructive sleep apnoea may be present.
Common causes of daytime mouth breathing in kids
✓ Blocked nose from allergies and colds
Frequent viral infections are a common part of childhood and each episode can cause swelling and excess mucus inside the nose. Children in childcare and primary school in Melbourne can have many colds each year, and if the nose never feels completely clear between episodes a pattern of mouth breathing can develop. The child simply finds it easier to get air in through the mouth.
Allergic rhinitis or hay fever is another major cause. In Victoria, triggers can include dust mites, grasses, pollens, animal dander and moulds. In allergic rhinitis the lining of the nose is chronically inflamed and swollen. Children may rub their nose, sneeze, sniff, have watery or blocked noses and dark circles under the eyes. This persistent narrowing of the nasal passages encourages mouth breathing both day and night.
✓ Enlarged adenoids and tonsils
The adenoids sit high at the back of the nose and the tonsils sit further down at the back of the throat. In many children these tissues are relatively large and play a role in the immune system. Sometimes they become so enlarged that they physically narrow the airway.
When adenoids are very big they can obstruct the back of the nose. The child may sound as though they always have a blocked nose, breathe with the mouth open and snore at night. Enlarged tonsils can narrow the throat and contribute to snoring, noisy breathing and obstructive sleep apnoea. Many children referred to Melbourne ENT with mouth breathing and snoring are found to have significantly enlarged adenoids, tonsils or both.
✓ Structural nasal issues
Some children have structural differences in the nose that make nasal breathing difficult. The septum, which divides the nose into left and right sides, may be deviated so that one or both sides are narrowed. The turbinates, which are normal structures that warm and filter the air, can become chronically enlarged. Prior nasal injuries, such as from sport, falls or accidents, can also alter the internal shape of the nose.
These issues are often considered in older children and teenagers, particularly when there is a history of trauma or long standing difficulty in breathing through one side of the nose. An ENT assessment can help determine whether these structural problems contribute substantially to mouth breathing and whether treatment is best directed at medical management, surgery in later adolescence or a combination.
✓ Habitual mouth breathing and posture
Sometimes mouth breathing starts as a reasonable response to a blocked nose during an infection or allergy flare and then simply never fully switches off. The child continues to rest with an open mouth even after congestion improves. Habitual mouth breathing can be reinforced by low tongue posture, prolonged dummy use, thumb sucking and head forward posture during long periods of screen time.
While habit is part of the picture, there is often still some underlying airway sensitivity or obstruction. This is why ENT surgeons like Dr Simon Braham at Melbourne ENT often work together with dentists, orthodontists and speech pathologists. Medical treatment can improve airflow, while functional therapies can help retrain tongue position, lip seal and swallowing patterns.
Mouth breathing, snoring and sleep disordered breathing
✓ What is snoring and sleep disordered breathing?
Snoring occurs when air flows through a partially narrowed upper airway and causes soft tissues to vibrate. In children this narrowing commonly involves the soft palate, adenoids and tonsils but the nose can be involved as well. Snoring can be soft and occasional or loud and frequent.
Sleep disordered breathing describes a spectrum of breathing disturbances during sleep. At the mild end there may be simple snoring without clear pauses in breathing. At the more severe end is obstructive sleep apnoea, where the airway repeatedly narrows or closes. This can lead to drops in oxygen levels, increased work of breathing and fragmented sleep, even if the child does not fully wake.
✓ Why daytime mouth breathing plus snoring matters
When a child has both daytime mouth breathing and regular snoring, it suggests that their airway is under strain both during wakefulness and during sleep. Instead of nasal breathing being the relaxed default, the child depends heavily on the mouth to obtain enough air. This combination is one of the patterns that prompts GPs in Melbourne to refer to an ENT clinic such as Melbourne ENT.
At Melbourne ENT, Dr Simon Braham considers the frequency and loudness of snoring, any observed pauses or gasps, how the child behaves and learns during the day and whether there are signs of nasal or throat obstruction. Not every snoring child has obstructive sleep apnoea, but daytime mouth breathing and nightly snoring together make it particularly important to rule out significant sleep disordered breathing.
✓ Possible impacts on behaviour, learning and mood
Poor quality sleep can show up in individual children in many different ways. Some appear obviously sleepy, struggle to wake in the morning and want to nap or rest more than their peers. Others may be irritable, emotional or quick to anger. Some are described as “bouncing off the walls” or unable to sit still or concentrate, which can sometimes overlap with symptoms of attention deficit disorders.
Teachers may notice that the child has difficulty focusing, daydreams in class, falls behind with schoolwork or is more disruptive than usual. Parents may feel that their child is very different from how they expected them to be at this age. When these concerns occur in a child who also mouth breathes and snores, it raises the possibility that improving sleep and breathing might help. It is important to note that results vary between children and no medical or surgical treatment can guarantee a particular change in behaviour or academic performance.
How mouth breathing can affect growth, teeth and facial development
✓ Mouth breathing and dental crowding
Long term mouth breathing can influence how the jaws and teeth develop. With the lips open and the tongue sitting low in the mouth, the normal balance of pressure between the tongue, cheeks and lips changes. This can lead to a narrower upper jaw and contribute to crowded or crooked teeth, crossbite or open bite. Some children also develop a high, narrow palate.
Dentists and orthodontists in Melbourne frequently notice these patterns and ask about snoring, mouth breathing and sleep. When they suspect that airway issues are contributing, they often recommend an ENT review so that any nasal or throat problems can be addressed alongside orthodontic planning.
✓ Facial growth and the so called “adenoid facies”
In longstanding cases, mouth breathing has been associated with a particular facial growth pattern sometimes called “adenoid facies“. Features can include a longer appearing face, narrow upper jaw, flattened midface and a habitual open mouthed posture. Not every child with mouth breathing develops this appearance and many factors, including genetics, play a role in facial growth.
However, the possibility of altered facial development is one of the reasons early assessment is encouraged when mouth breathing is persistent and associated with snoring or other airway symptoms. Treating significant obstruction may help create better conditions for normal growth, although it is never possible to promise a specific change in facial appearance.
✓ Team based care with dentists and orthodontists
Best care for a child with mouth breathing often involves a team. GPs, paediatricians, ENT specialists, dentists, orthodontists and speech pathologists may all contribute to the assessment and management plan. At Melbourne ENT, Dr Simon Braham regularly communicates with dental and orthodontic colleagues across Melbourne and regional Victoria.
For example, an orthodontist might plan to widen a narrow upper jaw while the ENT specialist deals with enlarged adenoids or nasal allergy. Speech pathologists or myofunctional therapists might help a child learn to keep their tongue in a better position and develop a more efficient swallowing pattern. This coordinated approach aims to support both airway function and craniofacial development.
When should parents seek medical advice?
✓ Start with your GP or paediatrician
If you are worried about your child’s breathing, snoring or sleep, speaking with your GP or paediatrician is a sensible first step. It can be helpful to describe when you notice mouth breathing most often, how long it has been present and whether there are concerns about snoring, restless sleep, waking, school performance or behaviour. Some parents find it useful to take a short video of their child sleeping to show breathing patterns more clearly.
In Victoria, GPs usually coordinate referrals to specialists. After taking a history and examining the nose, throat, ears and chest, your GP can advise whether referral to an ENT surgeon such as Dr Simon Braham at Melbourne ENT is appropriate or whether other investigations should be considered first.
✓ When a referral to an ENT specialist is often considered
Referral to an ENT specialist is often considered when mouth breathing has been present for several months, when snoring occurs on most nights or when there are observed pauses or gasping during sleep. Concerns about growth, learning or behaviour that may be related to poor quality sleep are also important. Recurrent ear infections, hearing loss or glue ear in a mouth breathing child may indicate enlarged adenoids that require assessment.
Some children, particularly those with complex medical conditions, may be managed through tertiary centres such as the Royal Children’s Hospital or the Royal Melbourne Hospital. Many others with common ENT conditions are assessed and treated in specialist practices like Melbourne ENT or in conjunction with hospitals such as the Royal Victorian Eye and Ear Hospital. The specific pathway depends on the child’s needs and local referral arrangements.
What to expect at an ENT assessment
✓ Taking a detailed history
At an ENT consultation you can expect a detailed discussion about your child’s symptoms. The specialist will ask about mouth breathing, snoring, breathing pauses, restless sleep, nightmares, bedwetting, daytime tiredness and behaviour changes. They will also ask about infections, allergies, asthma, other medical conditions and any previous operations.
At Melbourne ENT, Dr Simon Braham aims to understand how your child’s breathing is affecting daily life at home, at school and in activities. This information helps to decide which tests are appropriate and what options might be most suitable.
✓ Examination of the nose, throat and ears
A careful examination of the nose, throat and ears is an important part of the assessment. The ENT specialist will look at the size and appearance of the tonsils, the shape of the nasal passages and any signs of allergy or chronic congestion. The ears are checked for signs of infection or middle ear fluid that could affect hearing.
Most children tolerate this examination well, especially when they are prepared and supported. At Melbourne ENT, efforts are made to create a calm, child friendly environment so that young patients and their families feel as comfortable as possible.
✓ Additional tests when needed
In some situations extra tests are helpful. A small flexible camera can sometimes be used in older children to look at the back of the nose and assess the adenoids. Hearing tests may be arranged if there is concern about recurrent ear infections or hearing loss. If obstructive sleep apnoea is suspected, a sleep study may be recommended to measure breathing, oxygen levels and sleep quality overnight.
Not all children need these tests. The decision is based on the severity of symptoms, the findings on examination and the child’s age and tolerance. The benefits and practicalities of each test are discussed with parents before they proceed.
✓ How Melbourne ENT approaches assessment
Melbourne ENT takes an individualised approach to every child. Dr Simon Braham considers the full combination of symptoms, examination findings and test results and explains them in clear, plain language. Parents are encouraged to ask questions and to take time to understand what is happening in their child’s airway.
Where appropriate, Melbourne ENT communicates with your GP, paediatrician, dentist or other specialists to ensure that everyone involved in your child’s care has a shared understanding of the plan. The aim is to help families feel informed and supported, not rushed or pressured.
Treatment options for daytime mouth breathing and related airway problems
✓ Non surgical and medical treatments
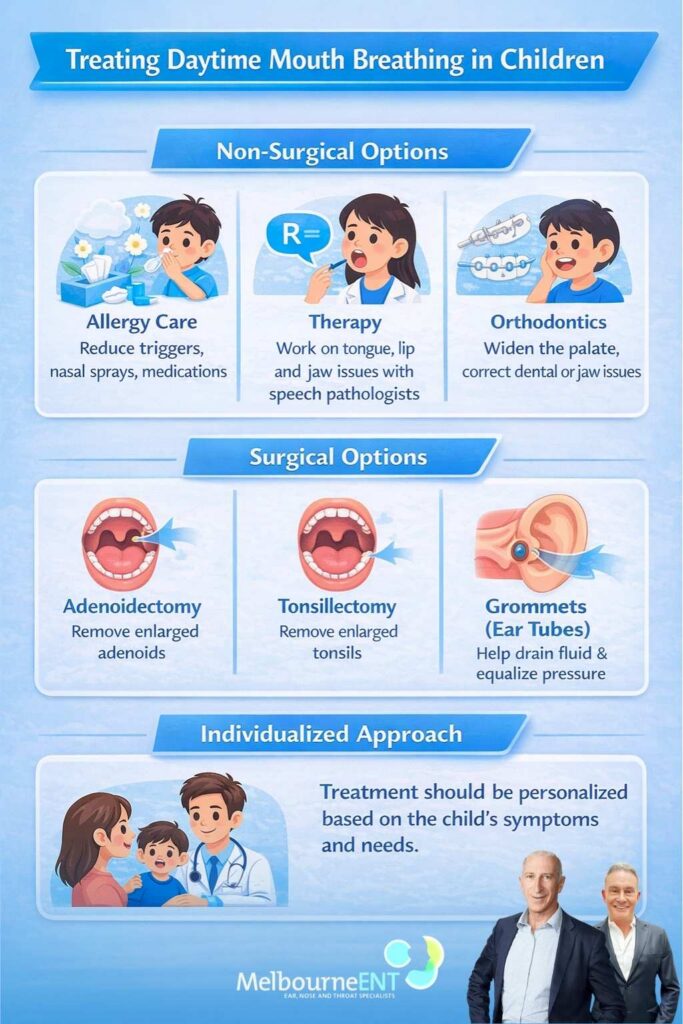
For many children the first steps are non surgical. When allergies are involved, treatment may include reducing exposure to triggers, using saline sprays or rinses and prescribing nasal corticosteroid sprays or antihistamines when appropriate. Good allergy control can make a noticeable difference to nasal airflow and comfort.
For children whose mouth breathing has developed around frequent colds, time, monitoring and supportive care may be all that is needed, provided there are no signs of significant sleep disordered breathing. Habitual mouth breathing can sometimes be improved with guidance from speech pathologists or myofunctional therapists who work on tongue posture, lip seal and swallowing. Dentists and orthodontists may recommend appliances or treatments to address narrow jaws or crowded teeth.
✓ Surgical options when they may be considered
Surgery is considered when there is clear evidence that structural obstruction is causing significant breathing and sleep problems and when non surgical measures have not been enough. Common operations include adenoidectomy, where enlarged adenoids are removed to improve airflow at the back of the nose, and tonsillectomy, often combined with adenoid surgery, when enlarged tonsils contribute to obstructive sleep apnoea or major sleep disordered breathing.
Grommets, or ventilation tubes, may be recommended for children with persistent middle ear fluid or recurrent ear infections that affect hearing. In selected older children and teenagers with marked structural nasal obstruction, nasal surgery such as septoplasty or turbinate reduction may be considered, usually once facial growth is more advanced. These decisions are always individual and involve detailed discussion of expected benefits, limitations and possible risks.
✓ Individualised planning and realistic expectations
Each child is different. At Melbourne ENT, Dr Simon Braham looks at the severity of symptoms, the impact on daily life, the results of any investigations and the child’s overall health before recommending treatment. In some cases careful observation and medical treatment are appropriate, while in others surgery may offer meaningful improvement in breathing and sleep.
It is important for families to understand that while many children improve after appropriate treatment, outcomes vary. No specific result can be guaranteed and there may still be a need for ongoing monitoring, dental care or behavioural support. Open discussion about goals and concerns helps ensure that decisions are made in a way that suits each child and family.
Medicare coverage, private health insurance and costs
In Australia, many ENT consultations and procedures for children attract Medicare rebates when there is a valid referral from a GP or other medical specialist and when clinical criteria are met. Medicare usually covers part of the cost of specialist appointments and eligible operations, with families paying any gap between the scheduled rebate and the actual fees charged. If surgery is carried out in a private hospital, private health insurance may contribute to hospital and theatre costs depending on the level of cover and waiting periods, while uninsured families need to consider the full hospital fees.
At Melbourne ENT, parents are given information about fees, item numbers and estimated out of pocket costs before they decide about surgery so that there are no surprises. Some children, especially those with complex needs, may have surgery arranged in public hospitals such as the Royal Children’s Hospital, the Royal Melbourne Hospital or the Royal Victorian Eye and Ear Hospital, where funding and waiting time arrangements differ. It is always reasonable to ask questions about financial aspects and to contact Medicare or your health fund for detailed information about rebates and coverage.
Risks, benefits and shared decision making
✓ Balancing the risks of surgery and the risks of not treating
All surgical and invasive procedures involve risks. For operations such as tonsillectomy, adenoidectomy or grommet insertion, potential complications can include pain, bleeding, infection, anaesthetic risks and in rare cases more serious problems. These risks depend on the child’s age, general health and the exact procedure and will be discussed thoroughly with the ENT surgeon.
There are also risks in leaving significant airway problems untreated. Ongoing obstructive sleep apnoea or severe sleep disordered breathing may affect behaviour, learning, growth and family life. In some situations the potential benefits of improving breathing and sleep outweigh the risks of surgery. In others a more conservative approach is appropriate. Careful assessment and discussion help families weigh these factors in a way that makes sense for them.
✓ Discussing options with your specialist
Shared decision making means that parents and specialists work together. You are encouraged to ask about the reasons for each recommendation, the likely recovery time, the expected impact on breathing and sleep and what to watch for during recovery. It is entirely acceptable to seek clarification if something is unclear or to request more time to think.
Some families choose to seek a second opinion from another appropriately qualified health practitioner, and this can sometimes provide extra confidence. At Melbourne ENT, Dr Simon Braham supports open conversation about options and respects the decisions that families make once they are fully informed.
Supporting your child at home
✓ Practical steps while waiting for appointments or tests
While waiting for appointments or tests there are several practical steps you can take. Keeping a simple sleep diary can be useful, noting how often your child snores, whether you see pauses or gasps and how they behave the next day. Short video clips of sleep can give your GP or ENT specialist valuable insight into what happens overnight.
You can also focus on general sleep hygiene. A regular bedtime routine, a quiet bedroom, limited screens before bed and avoidance of cigarette smoke can help many children. If allergies are part of the problem, dust reduction, washing bedding in hot water, keeping pets out of the bedroom and following the allergy plan recommended by your doctor may reduce symptoms while you are waiting for specialist review.
✓ Helping children feel comfortable with assessment and treatment
Children cope better with medical visits when they understand in simple terms what will happen. You might explain that they are going to see a nose and throat doctor who will look in their mouth, ears and nose to help them breathe more easily. Reassure them that many other children visit ENT clinics and that staff are used to helping kids feel safe and cared for.
If surgery is recommended, talking calmly about the plan can reduce anxiety. You can describe staying in hospital for a short time, having a special sleep with an anaesthetic doctor and then coming home to rest with soft foods and medicines for pain relief. At Melbourne ENT, the team aims to provide clear information to both children and parents and to support families coming from across Melbourne and regional Victoria.
FAQs About Daytime Mouth Breathing in Kids
Can daytime mouth breathing ever be part of normal development and then settle on its own?
There are times when mouth breathing is more of a temporary phase, particularly in younger children who are having many colds or mild nasal allergies. As infections settle and the nose clears, some children naturally return to comfortable nasal breathing without any specific treatment. If you are seeing mouth breathing on most days over several months, especially when your child otherwise seems well, it is sensible to have this checked so that an airway problem is not overlooked.
If my child seems moody or “in their own world“, could that be related to mouth breathing even if they do not look tired?
Daytime effects of poor sleep are not always obvious sleepiness. Some children with disturbed breathing at night appear more irritable, emotional or withdrawn rather than simply drowsy. Others can seem daydreamy, distracted or hard to motivate. While these changes can have many causes, mouth breathing and snoring are clues that sleep quality might be affected. It is worth discussing this combination of behaviour and breathing with your GP, who can decide whether referral to an ENT specialist such as Dr Simon Braham at Melbourne ENT would be helpful.
My child only mouth breathes when concentrating on screens or homework. Is that still a concern?
Parents often notice mouth breathing most when a child is deeply focused and their face is still, for example during screen time or homework. If the mouth is only slightly open occasionally and there are no issues with snoring or sleep, it may be less concerning. If your child regularly rests with the lips apart during quiet activities and you also notice snoring, restless sleep or a blocked sounding voice, it is reasonable to treat this as a possible sign of airway narrowing rather than just a concentration habit.
Will correcting mouth breathing change how my child’s face looks?
Chronic mouth breathing can influence jaw growth and dental alignment in some children, which is why early assessment is often recommended. Treating significant obstruction, such as enlarged adenoids or tonsils, may help support more normal patterns of growth and function. However, facial appearance is shaped by many factors, including genetics, and no treatment can guarantee a particular cosmetic change. At Melbourne ENT the focus is on improving breathing, sleep and general health, and any change in facial appearance is viewed as a possible secondary effect rather than a primary goal.
Do children grow out of enlarged adenoids and tonsils, and is it safe to wait?
Adenoids and tonsils do tend to change with age and can become less prominent in later childhood and adolescence. In children with mild symptoms, careful monitoring over time can be a reasonable option. In others, especially those with clear obstructive sleep apnoea, significant snoring or poor growth, the impact of waiting may outweigh the potential benefit of natural improvement. Decisions about whether to watch and wait or proceed with treatment are best made with an ENT specialist who can examine your child and discuss the likely risks and benefits for your specific situation.
Is it a good idea to tape my child’s mouth at night to train nose breathing?
Mouth taping in children is not recommended without specialist advice. Taping the mouth can make it harder for a child to protect their airway if they feel they cannot breathe comfortably. It may also hide an underlying problem such as obstructive sleep apnoea rather than treating it. If you are worried that your child relies too much on mouth breathing, especially at night, it is safer to have their airway assessed by your GP and, if needed, by an ENT surgeon such as Dr Simon Braham at Melbourne ENT, instead of trying to force nose breathing with tape.
Can sport or exercise make mouth breathing worse or better in children?
During vigorous exercise it is normal for many children to breathe through both the nose and mouth to move enough air. What matters more is how they breathe at rest and during sleep. Some children with nasal obstruction find that they struggle more with fitness or prefer to avoid sport because they feel short of breath or blocked, which can be a sign that the airway needs attention. Others feel better overall with regular activity and may have fewer problems with congestion when underlying issues are mild. If coaches or teachers comment on unusual breathing during sport, this is useful information to share with your GP alongside any history of mouth breathing and snoring.
Medical References
- Effectiveness of the Er:YAG Laser in Snoring Treatment Based on Clinical Studies / Journal of Clinical Medicine – NIH PMC / https://pmc.ncbi.nlm.nih.gov/articles/PMC12194654/
- A Comparison of Snoring Changes With a Supine-Avoidance Alarm Versus CPAP / Journal of Sleep Research – NIH PMC / https://pmc.ncbi.nlm.nih.gov/articles/PMC12856120/
- Possible Predictors of Apneic-Events During Sleep / Sleep and Breathing – NIH PMC / https://pmc.ncbi.nlm.nih.gov/articles/PMC12904870/
- The Natural History of Obstructive Sleep Apnea: A Scoping Review / Sleep Medicine Reviews – NIH PMC / https://pmc.ncbi.nlm.nih.gov/articles/PMC12897078/
- Snoring Symptoms and Obstructive Sleep Apnea Risk Factors / Sleep Medicine – NIH PMC / https://pmc.ncbi.nlm.nih.gov/articles/PMC12239641/
- Mandibular Advancement vs Combined Airway and Positional Therapy for Primary Snoring / Journal of Clinical Sleep Medicine – NIH PMC / https://pmc.ncbi.nlm.nih.gov/articles/PMC11117146/
- Obstructive Sleep Apnea (Key Symptom: Snoring) / StatPearls – NCBI Bookshelf / https://www.ncbi.nlm.nih.gov/books/NBK459252/
Next steps if you are worried about your child’s breathing
Occasional mouth breathing is very common, especially during colds or allergy flares, and often settles without any special treatment. Persistent daytime mouth breathing, particularly when combined with regular snoring, disturbed sleep or concerns about behaviour, learning or growth, deserves proper medical review. These patterns can sometimes indicate underlying airway problems that may respond to medical or surgical management.
Parents in Melbourne and across Victoria who are concerned about their child’s breathing can start by speaking with their GP or paediatrician. Where appropriate, a referral to an ENT specialist such as Dr Simon Braham at Melbourne ENT in St Kilda East can then be arranged. With careful assessment, clear explanation and an individualised plan, many children can be supported to breathe and sleep more comfortably, while recognising that results differ from child to child.
For more information about assessment and treatment of mouth breathing, snoring and other ENT concerns in children, or to learn more about Melbourne ENT and the services offered, talk to your GP about a referral and visit the website. This article is general in nature and does not replace personalised medical advice from a qualified health professional who has assessed your child in person.
Further Reading
- Read more about Breathing Problem for Kids Melbourne – Also Known As Paediatric Sleep Disordered Breathing
- Read Melbourne ENT’s blog on Breathing Problems for Kids – Causes and Solutions
- Read Melbourne ENT’s blog on How to Prevent Kids Inhaling Foreign Objects (Under 3 Years)

Daytime Mouth Breathing in Kids – Is It a Sign of Airway Problems?
Many parents first notice daytime mouth breathing when they look at photos of their child…

When a Persistent Cough After Winter Needs an ENT Opinion
Winter in Melbourne often brings a wave of colds and flu. For most people, the…

Tonsillitis Myths: Why Ice Cream Is Not The Treatment
For many people who grew up in Melbourne and across Australia, and for many of…