Parotid cancers are malignant tumours that arise within the parotid gland, the largest of the salivary glands. This gland sits just in front of the ear and extends down towards the angle of the jaw. It wraps around the facial nerve, the nerve that controls the muscles of facial expression. Because of this close relationship, cancers in the parotid region require careful assessment and treatment by surgeons with head and neck cancer experience, as both cancer control and preservation of facial function are important considerations.
At Melbourne ENT in St Kilda East, Victoria, patients with parotid cancers are managed in a dedicated ear, nose, throat and head and neck surgery setting. Parotid cancer surgery is performed by ENT and head and neck surgeon Dr Stephen Kleid. He has extensive experience managing head and neck tumours, including cancers of the parotid gland, other salivary glands, thyroid, throat and mouth, in both public and private hospitals.
Parotid cancer surgery is a medically necessary procedure. It is not a cosmetic operation, although the impact on appearance and facial symmetry is taken into account where this can be done safely. The primary aim is to remove or reduce the cancer, protect vital structures such as the facial nerve and coordinate further treatments such as radiotherapy when appropriate. The information on this page is intended as a general guide only and does not replace advice from your own doctor or specialist.
What Is Parotid Cancer Surgery?
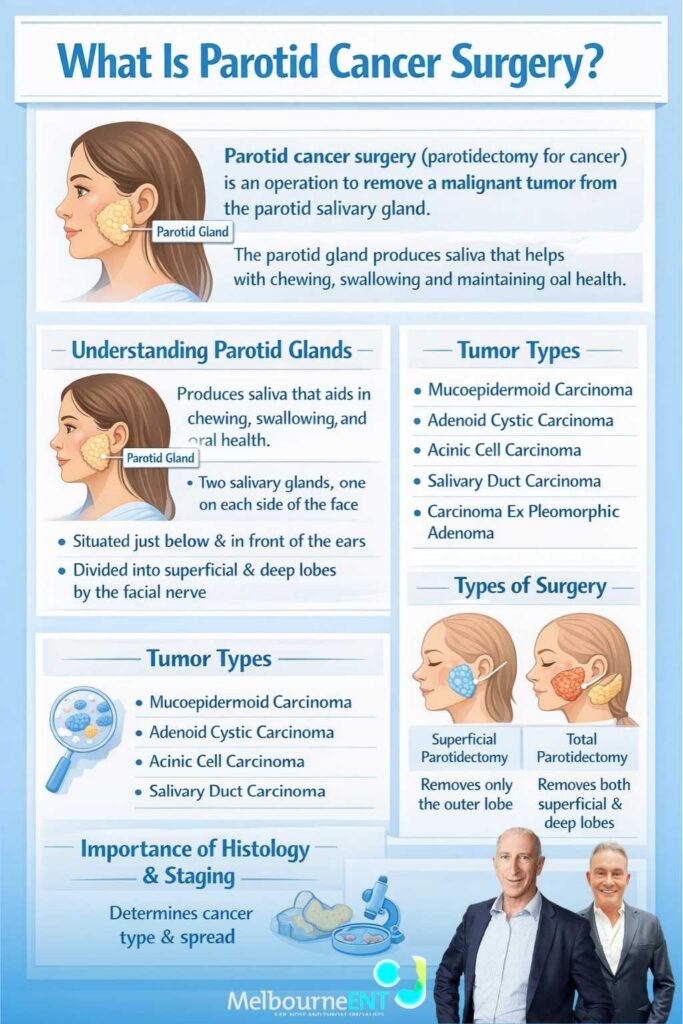
Parotid cancer surgery, sometimes referred to as parotidectomy for cancer or parotid gland cancer surgery, is an operation to remove a malignant tumour arising from the parotid salivary gland. The parotid gland produces saliva that helps with chewing, swallowing and maintaining oral health. Each person has two parotid glands, one on each side of the face, situated just below and in front of the ear, divided into superficial and deep lobes by the facial nerve that passes through them.
Most parotid lumps are benign. Common non-cancerous tumours include pleomorphic adenomas and Warthin tumours. However, a proportion of parotid tumours are malignant and are classified as parotid cancers or salivary gland carcinomas. These include a number of different tumour types, such as mucoepidermoid carcinoma, adenoid cystic carcinoma, acinic cell carcinoma, salivary duct carcinoma and carcinoma ex pleomorphic adenoma. Each type has its own behaviour and pattern of spread, which is why detailed histology and staging are so important.
Parotid cancer surgery generally involves removing the portion of the gland that contains the tumour and often the entire gland on that side. When the tumour is confined to the outer part of the gland, the procedure may be a superficial parotidectomy, in which only the superficial lobe is removed. For many parotid cancers, particularly those involving the deep lobe or those that are higher grade, a total parotidectomy, removing both superficial and deep lobes, is recommended. In some circumstances, tissues around the gland, such as skin, muscle or bone, may also need to be removed if they are directly involved by the cancer.
If there is evidence that lymph nodes in the neck are involved, or if the tumour type carries a high risk of spread to these nodes, a neck dissection may be performed at the same time. This involves removing specified lymph node groups in the neck to treat and stage the disease. Depending on the extent of surgery, reconstructive techniques may be used to support facial contour, protect the facial nerve and reduce the likelihood of problems such as Frey syndrome. Throughout, the overall focus is on safe, oncologically appropriate removal of the tumour and on gathering accurate information to guide any further treatment such as radiotherapy.
Who Needs It (Candidates For Parotid Cancer Surgery)?
Parotid cancer surgery is usually considered for patients with a confirmed diagnosis of malignancy in the parotid gland or a strong suspicion of cancer based on clinical assessment, imaging and needle biopsy. Many people initially present because they have noticed a lump in front of or below the ear, or at the upper part of the neck. This lump might have been present for some time and only recently started to grow, or it might have appeared relatively quickly.
Features that can raise concern for parotid cancer include a lump that feels firm, irregular or fixed to deeper tissues, a mass that steadily increases in size over weeks or months, or symptoms such as pain in the parotid region, fullness or discomfort near the ear, or pain referred into the ear itself. Some patients notice changes in facial movement, such as difficulty smiling evenly, drooping at one corner of the mouth, reduced ability to close one eye or reduced movement of the forehead on one side. Others become aware of numbness or altered sensation over the cheek, ear or jawline. Occasionally, the first sign is a lump in the upper neck that turns out to be a lymph node containing spread from a parotid tumour.
Investigations are an important part of determining who should have surgery. Ultrasound, CT and MRI scans can help define the size and location of the tumour, its relationship to the facial nerve and other structures, and whether lymph nodes appear involved. Fine needle aspiration or core biopsy is typically used to sample the lump and may suggest a specific tumour type or indicate that the lesion is likely to be malignant. In some cases, the biopsy result may be inconclusive or show features that are suspicious rather than definite, and surgery may be recommended both to remove the tumour and to allow full pathological assessment.
Suitability for surgery also depends on broader health factors. Age, general fitness, heart and lung health, previous surgery or radiotherapy in the area, and other medical conditions can all influence whether a major operation is advisable. In certain situations, such as when the cancer is very advanced or has spread widely, or when other health problems mean anaesthesia would be too risky, non-surgical treatments may be considered instead. Decisions about surgery are often made in a multidisciplinary setting, where surgeons, radiologists, pathologists, radiation oncologists and medical oncologists discuss the case together to plan the most appropriate approach.
Benefits Of Parotid Cancer Surgery
The potential benefits of parotid cancer surgery are primarily related to cancer control and accurate staging, but there can also be important benefits for symptom relief and long-term quality of life. Removing the primary tumour from the parotid gland helps reduce the risk of the cancer continuing to grow locally, invading surrounding structures and causing further damage to the facial nerve, skin or bone. In many cases, surgery is an essential step in attempting to control the disease in the region of the gland and neck.
When a neck dissection is performed as part of the operation, lymph nodes that already contain spread from the parotid cancer can be removed. This allows treatment of known nodal disease and may reduce the risk of further regional progression. Even when lymph nodes do not appear abnormal on examination or imaging, removing them in selected cases can provide additional information about microscopic spread that could influence decisions about radiotherapy.
Another major benefit of surgery is the detailed information that becomes available when the tumour and any involved lymph nodes are examined in full by a pathologist. Needle biopsies can provide important clues but are limited by the small amount of tissue obtained. Examination of the entire tumour allows more accurate determination of the exact tumour type, the grade or aggressiveness of the cancer, whether there is spread along small nerves or blood vessels, and whether the margins of resection are clear or close. This information helps guide decisions about post-operative radiotherapy and gives a clearer picture of the likely risk of recurrence.
For some patients, surgery also helps relieve symptoms such as pain, pressure and visible swelling. A growing parotid tumour can be uncomfortable, can interfere with wearing glasses or hearing aids and can become more conspicuous over time. While the primary goal of surgery remains cancer control, reduction of tumour bulk and improvement in local comfort can be important for day to day wellbeing. In carefully selected cases, reconstructive steps may also support facial symmetry and soften contour changes, acknowledging that complete restoration to a pre-illness appearance is not always possible.
The effect of surgery on facial movement, speech, chewing and swallowing is variable and depends on factors such as tumour size, extent of surgery and the degree to which the facial nerve can be preserved. Where the nerve is not directly involved by tumour and can be carefully dissected away, there is often a good chance of partial or substantial recovery of function over time, even if there is temporary weakness early on. Where a segment of the nerve must be removed, the goal may be to restore some degree of movement with nerve grafts or other reconstructive procedures, understanding that results differ between individuals and that realistic expectations are important. These likely outcomes, and the potential benefits and limitations of surgery in your own situation, are discussed in detail before any decision to proceed.
Consultation For Parotid Cancer Surgery
The consultation at Melbourne ENT for possible parotid cancer surgery is focused on understanding your diagnosis, clarifying your options and helping you decide on a plan that suits your medical needs and personal circumstances. For many patients, this is the first time discussing head and neck cancer in detail, and it is entirely normal to arrive with questions and worries.
During the consultation, Dr Stephen Kleid will ask about your symptoms and medical background. This includes when you first noticed the parotid lump, how quickly it has changed, whether you have pain, facial weakness or numbness, and whether there are any swallowing, speech or breathing difficulties. Your general health, past medical conditions, previous surgeries, current medications and allergies will also be reviewed, as these can influence both surgical risk and anaesthetic planning. A history of previous radiotherapy or cancer treatment is especially important to share.
A thorough examination of the head and neck follows. The parotid region and both sides of the face are inspected and gently felt to assess the size, consistency and mobility of the lump. Facial nerve function is carefully tested by asking you to raise your eyebrows, close your eyes tightly, smile, purse your lips and perform other facial movements. The mouth, tongue, palate and throat are examined, and the neck is checked for enlarged lymph nodes or other abnormalities.
Any imaging studies, such as ultrasound, CT, MRI or PET CT scans, are reviewed with you, and the findings are explained in everyday language. Fine needle aspiration or core biopsy results are also discussed, including any uncertainties or limitations in those results. If further tests or repeat imaging are advisable, this will be outlined.
Once all the available information has been assembled, Dr Kleid will discuss whether parotid cancer surgery is recommended in your situation and, if so, what type of operation is most appropriate. The discussion typically covers the likely extent of parotidectomy, any anticipated neck dissection, the possible need for reconstructive techniques, the potential role of post operative radiotherapy and the expected course of recovery. Risks and potential complications are explained, and you are encouraged to ask questions and take the time you need to process the information. Many patients find it reassuring to bring a family member or trusted friend to help listen and provide support.
If you decide to proceed with surgery, the practice staff assist with practical arrangements, including hospital booking, pre-operative tests and scheduling of follow-up appointments. You will also be given information about fees, Medicare rebates and private health insurance, so that you can make an informed decision not only medically but also financially.
How Is It Performed (Surgery For Parotid Cancers)?
Parotid cancer surgery is carried out in an accredited hospital under general anaesthesia. On the day of the operation, you are admitted to hospital and checked in by the nursing and anaesthetic teams. They confirm your details, review your medical history and ensure that fasting instructions and any medication changes have been followed. The anaesthetist explains the plan for anaesthesia, pain relief and post operative monitoring.
Once in the operating theatre and under general anaesthesia, the skin over and around the parotid gland and neck is prepared and draped in a sterile fashion. The surgeon marks out the incision, which is usually a curved line starting in front of the ear, passing around the earlobe and sometimes extending behind the ear and down into a natural crease in the neck. This pattern allows access to the parotid gland and the neck while helping to place the scar in areas that may blend more easily with natural skin lines as healing progresses.
The skin and underlying tissues are gently elevated to expose the parotid gland and the region where the facial nerve emerges from the skull. Identifying the facial nerve is a critical step. Magnification and fine instruments are used to locate the main trunk of the nerve and then trace its branches as they fan out through the gland. Throughout the dissection, the surgeon works carefully to preserve the nerve and its branches whenever this is safe from an oncological perspective. In some cases, nerve monitoring equipment is used as an additional aid, although the surgeon’s experience and knowledge of anatomy remain central.
Once the facial nerve has been identified and protected as far as possible, the diseased portion of the parotid gland is removed. In superficial parotidectomy, the outer lobe of the gland lying over the nerve is excised. In total parotidectomy, both the superficial and deep lobes are removed, which is often necessary for parotid cancers that are deep, large or high grade. The extent of gland removal is determined by the size and location of the tumour, its proximity to the nerve and the need to obtain adequate margins of apparently normal tissue around the cancer.
If imaging or findings at surgery indicate that lymph nodes in the neck are involved or at significant risk, a neck dissection is carried out through the same incision or a connected extension. This involves carefully removing specified groups of lymph nodes while preserving important surrounding structures such as major nerves and blood vessels. The type and extent of neck dissection are guided by established head and neck cancer principles and are tailored to the individual case.
In some situations, the tumour may be directly invading the facial nerve. When this occurs, achieving complete tumour removal may require sacrificing a segment or, rarely, the majority of the nerve on that side. If this is necessary, the surgeon may perform nerve reconstruction using a graft taken from another nerve in the body or by connecting remaining nerve segments to other functioning nerves. These techniques aim to restore some degree of facial movement over time, although they cannot fully replicate normal function. Adjunctive soft tissue reconstruction, such as using local muscle or tissue flaps or fat grafting, may also be undertaken to fill the defect, protect structures and help reduce hollowing.
At the end of the operation, a small drain is usually placed under the skin to remove fluid and reduce the risk of haematoma or fluid collection. The tissues are then closed in layers, and the skin is sutured or stapled. A dressing is applied over the incision. The duration of the surgery varies according to the complexity of the case, the need for neck dissection and reconstruction, and the individual’s anatomy. Dr Kleid will discuss expected operative time and the general sequence of events as part of the consent process.
Recovery After Parotid Cancer Surgery
Recovery from parotid cancer surgery takes time and progresses in stages. Immediately after the operation, you are taken to a recovery area where nurses and the anaesthetist closely monitor your breathing, blood pressure, oxygen levels, pain control and overall comfort. Once you are fully awake and stable, you are transferred to the ward.
Most patients remain in hospital for one to three nights, though this can vary depending on the extent of surgery and general health. During your hospital stay, you are encouraged to begin mobilising, sitting out of bed and walking short distances, as this helps reduce the risk of complications such as blood clots and chest infections. The drain near your incision is monitored regularly, and it is usually removed once the amount of fluid collected has dropped to an acceptable level. Pain is managed with regular tablets and, if necessary, additional medications, and the nursing staff keep a close eye on the wound and facial movement.
The first week or two at home is often a period of adjustment. Swelling and bruising around the ear, jaw and neck are common and may make the area feel tight or heavy. There is almost always some numbness or altered sensation around the ear and on the side of the face and neck, which can feel strange but is expected. Facial weakness may be present, particularly when trying to smile, raise the eyebrows or close the eye fully. When the facial nerve has been preserved, this weakness is often at least partly due to swelling and temporary nerve irritation and may improve gradually over the following weeks and months.
You will be given instructions about caring for the wound, including when it is safe to get the area wet and how to recognise signs of infection. Sleeping with your head slightly elevated can help reduce swelling, and it is usually recommended to avoid heavy lifting, strenuous exercise and contact sports for a period of time. Stitches or staples are typically removed or checked within the first week or so at a follow-up appointment. Your surgeon may then discuss scar care, such as gentle massage or the use of particular dressings or gels, once the incision has healed.
Over subsequent weeks, the swelling diminishes, and the scar becomes less prominent. Many people are able to return to desk-based work within a few weeks, while more physically demanding roles may require a longer recovery period. Fatigue is not uncommon after major surgery, and this can be more pronounced if radiotherapy is planned. If post operative radiotherapy is recommended based on the pathology findings, it is usually started once the wound has healed sufficiently, and you will be referred to a radiation oncology team to discuss this in detail.
Longer term, follow-up appointments with Dr Kleid allow review of the pathology report, assessment of facial nerve function, monitoring for signs of recurrence and support in managing any ongoing issues such as Frey syndrome, persistent numbness, eye closure difficulties or asymmetry. In some cases, referral to allied health professionals such as physiotherapists, speech pathologists, dietitians or psychologists may be helpful in supporting recovery of function, nutrition and emotional wellbeing. Parotid cancer treatment is rarely a single event; instead, it is usually a process that continues over months and requires regular monitoring.
Risks And Complications Of Parotid Cancer Surgery

Like all operations, parotid cancer surgery carries risks. Because the parotid gland is closely related to the facial nerve and other vital structures, there are specific considerations that need to be understood before proceeding. Dr Kleid will explain these risks in the context of your individual health, the nature of your tumour and the extent of surgery required.
General surgical risks include bleeding, infection and delayed wound healing. A collection of blood under the skin, known as a haematoma, can occasionally form and may require further drainage. As with any major surgery under general anaesthesia, there is a small risk of complications related to the anaesthetic, such as reactions to medications, heart or lung problems, or blood clots in the legs or lungs. Measures such as careful monitoring, early mobilisation and, where appropriate, preventive medications are used to reduce these risks.
The most significant specific risk for many patients is facial nerve weakness or paralysis. Even when the nerve is preserved, temporary weakness is common after surgery due to stretching, handling and swelling. This can affect the ability to close the eye, smile symmetrically, raise the eyebrows or move the lower lip. In many cases, particularly when the nerve has not been invaded by tumour, at least some recovery occurs over time. However, when a segment of the nerve has to be removed to achieve cancer clearance, permanent weakness in the affected part of the face is likely, even if nerve grafting or other reconstructive procedures are performed. Further operations or rehabilitative strategies may help improve appearance and function but cannot guarantee a full return to normal.
Numbness and altered sensation around the ear, cheek and neck are also very common after parotid surgery because small sensory nerves in this area are cut during the operation. Some patients experience tingling or sensitivity as nerves try to recover. For many people, the altered sensation becomes less noticeable with time, but in some cases it can be long-lasting. Another specific complication is Frey syndrome, in which the skin over the cheek or temple becomes red, warm and sweaty when eating or thinking about food. This occurs because nerves that previously supplied the salivary gland reconnect with sweat glands in the skin. Frey syndrome is not dangerous but can be bothersome; topical treatments or injections may help reduce symptoms.
A salivary fistula, where saliva leaks under the skin or through the wound, can occur after parotidectomy. This often settles with dressings, pressure and time, although occasionally additional treatment is required. Cosmetic considerations include a visible scar around the ear and possibly into the neck, and hollowing or contour change where the gland has been removed. While scars often fade and soften over time and can be partly hidden in skin creases, this process varies between individuals, and some contour change is common after removal of a substantial gland.
Despite appropriate surgery and, where indicated, radiotherapy, there remains a risk that parotid cancers can recur either in the area of the parotid bed, in lymph nodes or elsewhere in the body. The likelihood of recurrence depends on many factors, including tumour type, grade, margin status and nodal involvement. Regular follow-up and ongoing surveillance with clinical review and, when appropriate, imaging are therefore vital parts of long term care. Dr Kleid will outline which risks are particularly relevant for you and explain the strategies used to reduce them as far as possible.
Cost Of Parotid Cancer Surgery
The overall cost of parotid cancer surgery varies from patient to patient. It is influenced by the complexity and duration of the operation, whether a neck dissection or reconstructive procedures are needed, the hospital where surgery is performed, and the fees charged by the surgeon, anaesthetist and hospital. Your private health insurance status and level of cover, along with any excesses or co-payments, also play a role in determining out of pocket expenses.
At Melbourne ENT, there is an emphasis on providing clear information about fees before you decide to proceed. As part of the informed financial consent process, you are usually given a written estimate of the surgeon’s fees and an indication of the expected Medicare rebate and, if applicable, private health fund contribution. You may also receive details about likely anaesthetic and hospital fees or be given item numbers that you can quote to your health fund to clarify what is covered. This allows you to understand the likely financial implications and ask questions before committing to surgery.
Because Medicare rebates, health fund policies and provider fees can change over time, and because each person’s circumstances are different, specific dollar amounts are not listed here. If you have concerns about costs or financial constraints, it is important to raise these with the practice staff. In some cases, the timing of surgery, the choice of hospital or alternative treatment approaches may need to be considered in light of both medical and financial factors, and these discussions should occur openly and without pressure.
Medicare Coverage And Insurance
Parotid cancer surgery is a medically necessary procedure rather than an elective cosmetic operation. In most cases, it is associated with one or more Medicare item numbers, which means that Medicare pays a portion of the surgeon’s and anaesthetist’s fees. If you hold private hospital insurance, your health fund may also contribute to hospital and theatre charges, depending on the details of your policy.
The amount covered by your health fund will depend on the level of cover you have selected, any waiting periods or exclusions that apply and whether an excess or co-payment is due. Some policies provide comprehensive cover for hospital and theatre fees, while others may leave a larger gap for you to pay personally. Even with insurance, there may still be out of pocket costs, often referred to as gaps, reflecting the difference between the total fees and the combined Medicare and health fund rebates.
Before surgery, you are usually provided with the relevant item numbers and encouraged to contact your health fund to confirm what is covered in your situation. This includes asking whether your policy covers the planned procedure, whether there are any restrictions related to pre-existing conditions or waiting periods, what excess or co-payments might apply and whether your choice of hospital affects your entitlement. The staff at Melbourne ENT can assist in guiding you towards the right questions to ask, but only your health fund can give detailed, up to date information about your individual policy.
Why Choose Your Surgeon
When facing a diagnosis of parotid cancer, many people wish to be treated by a surgeon with specific experience in head and neck cancer. At Melbourne ENT, parotid cancer surgery is performed by ENT and head and neck surgeon Dr Stephen Kleid. He is a Fellow of the Royal Australasian College of Surgeons and has many years of experience managing a broad range of head and neck tumours, including cancers of the parotid gland, other salivary glands, thyroid, throat and mouth, in major Melbourne hospitals as well as in private practice.
Dr Kleid’s training and practice include dedicated work in head and neck tumour surgery. His approach to parotid cancers is based on established oncological principles, with an emphasis on removing the tumour with appropriate margins where possible while paying close attention to preserving the facial nerve and other critical structures whenever it is safe to do so. When necessary, reconstructive techniques are incorporated into the surgical plan to support facial function and improve contour, recognising that the primary goal remains effective treatment of the cancer.
Melbourne ENT is structured to provide coordinated care from the point of first consultation through surgery and into long-term follow-up. Where appropriate, cases are discussed with other specialists, including radiologists, pathologists, radiation oncologists and medical oncologists, as part of a multidisciplinary approach to head and neck cancer care. This allows treatment decisions, such as the use of post operative radiotherapy or systemic therapies, to be made in a collaborative manner.
Patients are encouraged to ask questions, bring a support person to appointments and take time to consider their options. The practice aims to provide clear explanations, realistic expectations and ongoing support during what can be a challenging time. If you would like more information about Dr Kleid’s background, experience and interests within ENT and head and neck surgery, further details are available from the Melbourne ENT practice.
FAQs About Parotid Cancer Surgery
Can parotid cancer or its treatment affect how food and drink taste, and if so, does this usually improve over time?
Changes in taste can occur after parotid cancer treatment. This may be related to altered saliva production, minor nerve changes in the area or, in some cases, radiotherapy if it is required. Many people notice gradual improvement over several months as healing progresses, although taste may not always return exactly to how it was before. If taste changes are bothering you, Dr Kleid and your broader care team can suggest strategies to keep eating enjoyable and maintain good nutrition.
Will I still make enough saliva after surgery on one parotid gland, or is there a risk of long-term dryness in the mouth or throat?
Most people still produce enough saliva after removal of one parotid gland because the remaining salivary glands can often compensate to a degree. Some patients notice mild dryness, particularly if radiotherapy is also needed, or at night when saliva production is lower. Simple measures such as sipping water regularly, using sugar-free gum or lozenges and maintaining good dental care can be helpful. If dryness is significant or persistent, this can be discussed with Dr Kleid so that additional options can be considered.
If my facial nerve is bruised but not cut during surgery, what subtle changes in expression or eye closure should I look out for in the first few months?
When the facial nerve is stretched or bruised but not divided, you may notice mild asymmetry when you smile, a slightly weaker blink on the operated side or a feeling that the face becomes more tired as the day goes on. Sometimes the lower lip can pull a little differently, or the eyebrow movement is not quite as strong as before. These changes often improve gradually as the nerve recovers, although the timeline varies between individuals. If you notice new or worsening weakness, it is important to let Dr Kleid know so that it can be assessed.
How might parotid cancer surgery and possible radiotherapy affect future dental work, and should I see my dentist before treatment starts?
Parotid surgery and especially radiotherapy can influence saliva flow and the condition of the teeth and jaws over time. Reduced saliva can increase the risk of tooth decay, and previous radiotherapy in the area can affect how the jawbone heals after certain dental procedures. It is usually wise to see your dentist before treatment begins to address any existing dental issues and to plan ongoing care. Dr Kleid can work together with your dentist and, if needed, a radiation oncologist to help coordinate safe and appropriate dental management.
Are there specific sleeping positions, pillows or supports that can make it safer or more comfortable to rest in the first weeks after surgery?
In the early weeks after surgery, many patients find it more comfortable to sleep with the head slightly elevated on extra pillows or a wedge pillow to help reduce swelling. Resting on the side opposite to the operation often feels easier and avoids direct pressure over the wound and drain site. A small, soft pillow or rolled towel can be used to support the neck and shoulder so that the head does not roll onto the operated side during the night. If you are unsure about what is suitable for your situation, this can be discussed with Dr Kleid or the hospital nursing staff before you leave hospital.
Once treatment is finished, what sort of self-check or routine should I follow at home to notice possible signs of recurrence between follow-up visits?
After treatment, it can be helpful to become familiar with how your face, scar and neck feel so that you can notice any changes. From time to time, you might gently feel along the scar and around the neck for new lumps, watch in the mirror for any new facial weakness or asymmetry and pay attention to new or persistent pain, swallowing difficulties or unexplained weight loss. These checks are not a substitute for regular follow-up with Dr Kleid but can help you recognise changes earlier. If you notice anything that concerns you, it is important to raise it at your next appointment or contact the practice for advice.
If I am feeling anxious or low after a cancer diagnosis and surgery on my face, what kinds of support or rehabilitation services are usually available to help with adjustment and confidence?
Feeling anxious, low or self-conscious after a cancer diagnosis and surgery in a visible area is very common. Support can come from several sources, including your GP, Dr Kleid, hospital-based social workers, psychologists with experience in cancer care and community support groups. In addition, physiotherapists, speech pathologists and occupational therapists may help with facial movement, swallowing, speech or practical adjustments, which can also improve confidence over time. If your mood or coping is worrying you, it is important to mention this so that you can be linked with appropriate support rather than managing alone.
Medical References:
- Parotid Cancer. NCBI Bookshelf. Updated May 2023.
https://www.ncbi.nlm.nih.gov/books/NBK538340/ - Mucoepidermoid carcinoma of the parotid gland: factors affecting outcome.
https://pubmed.ncbi.nlm.nih.gov/20629088/ - Management of Salivary Gland Malignancy. Journal of Clinical Oncology.
https://ascopubs.org/doi/10.1200/JCO.21.00449 - Neck Dissection for Salivary Gland Malignancies.
https://pmc.ncbi.nlm.nih.gov/articles/PMC6405234/ - Metastatic cutaneous squamous cell carcinoma to the parotid: the role of surgery and adjuvant radiotherapy.
https://pubmed.ncbi.nlm.nih.gov/12956783/
Book An Appointment
Being told you have a parotid tumour or parotid cancer can be unsettling. It is normal to feel uncertain and to want clear, trustworthy information about what comes next. Speaking with an experienced ENT and head and neck surgeon can help you understand your diagnosis, explore your options and make decisions that are appropriate for your health, your values and your circumstances.
If you have been diagnosed with parotid cancer, have a persistent or enlarging lump near the ear or upper neck, or have been advised to seek a specialist opinion about a parotid lump, you can talk to your general practitioner or referring doctor about obtaining a referral to Melbourne ENT in St Kilda East, Victoria, for assessment by Dr Stephen Kleid. A referral usually allows Medicare rebates to apply to your consultation and helps ensure that your GP and specialist can communicate clearly about your care.
Once a referral has been arranged, you can contact Melbourne ENT to discuss appointment availability, which scans and test results to bring and any questions you may have about the consultation or possible surgery. Many patients find it helpful to write down their questions beforehand and to bring a family member or close friend for support.
The information on this page is general and cannot cover every individual situation. It does not replace personalised advice from your own doctor or specialist. For guidance that takes into account your specific diagnosis, medical history and personal priorities, it is important to consult directly with Dr Kleid, your GP or your treating cancer team and to work together on a plan that is right for you.
Further Reading
- Read about Melbourne ENT’s Head And Neck Cancer Surgery
- Read about Melbourne ENT’s Thyroidectomy Melbourne – Also Known As Thyroid Cancer Surgery
- Read about Melbourne ENT’s Parotidectomy Melbourne – Also Known As Parotid Gland Surgery
- Read about Melbourne ENT’s Goitre Surgery Melbourne – Also Known As Thyroid Surgery