

Breathing through the nose is something many people do without thinking. When it is working well, nasal breathing is usually quiet, steady and comfortable. The nose filters, warms and humidifies the air before it reaches the throat and lungs. It also contributes to normal upper airway function and can affect how a person sleeps, rests and breathes during daily activity.
When nasal breathing is difficult, many people compensate by breathing through the mouth. This may happen during a cold, after exercise, or during a short flare-up of hay fever. For some adults and children, however, mouth breathing becomes a regular pattern.
Chronic mouth breathing is not always a sign of a serious medical condition. However, when it is persistent, especially during sleep, it may be associated with nasal obstruction, allergies, enlarged adenoids, enlarged tonsils, sinus inflammation, snoring, sleep-disordered breathing or other upper airway concerns.
At Melbourne ENT in St Kilda East, Victoria, Dr Simon Braham MBBS (Hons), FRACS, ENT and Head and Neck Surgeon, sees adults and children with blocked nasal breathing, mouth breathing, snoring, sleep disturbance and related ear, nose and throat concerns. The purpose of assessment is to understand the likely cause of symptoms and discuss treatment options that may be suitable for the individual patient.
Melbourne ENT’s approach is based on careful assessment, clear explanation and individualised care. Treatment may involve medical management, allergy care, sleep assessment, dental or allied health input, or surgery when clinically appropriate.
Why Nasal Breathing Matters
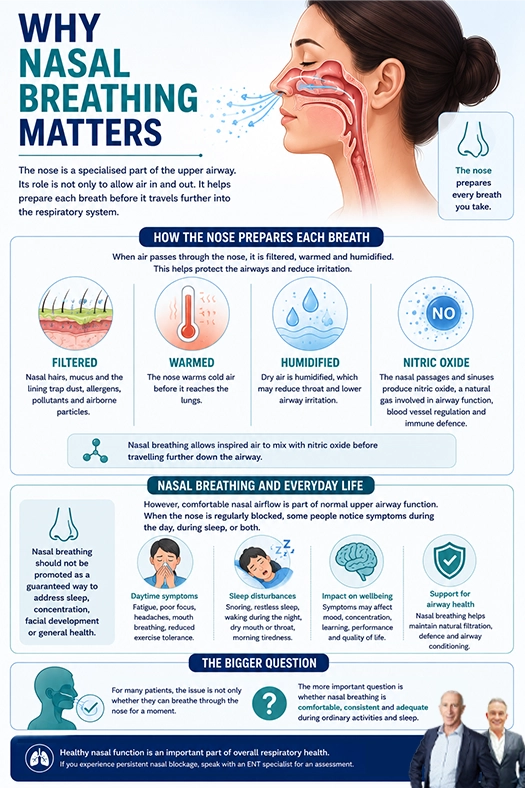
The nose is a specialised part of the upper airway. Its role is not only to allow air in and out. It helps prepare each breath before it travels further into the respiratory system.
When air passes through the nose, it is filtered by nasal hairs, mucus and the lining of the nasal passages. These structures help trap dust, allergens, pollutants and airborne particles. The nose also warms cold air and humidifies dry air, which may reduce irritation in the throat and lower airway.
The nasal passages and sinuses also contribute to the production of nitric oxide, a naturally occurring gas involved in airway function, blood vessel regulation and immune defence. Nasal breathing allows inspired air to mix with nitric oxide before travelling further down the airway.
Nasal breathing should not be promoted as a guaranteed way to address sleep, concentration, facial development or general health. However, comfortable nasal airflow is part of normal upper airway function. When the nose is regularly blocked, some people notice symptoms during the day, during sleep, or both.
For many patients, the issue is not only whether they can breathe through the nose for a moment. The more important question is whether nasal breathing is comfortable, consistent and adequate during ordinary activities and sleep.
How The Body Supports Nasal Breathing
At rest, most people are naturally suited to breathing through the nose. The nose, sinuses, palate, tongue and throat all work together as part of the upper airway.
When nasal breathing is comfortable, the lips are more likely to rest together, and the tongue commonly rests against the palate. This resting posture may support normal oral function. In children, breathing patterns may interact with facial muscle balance, jaw posture and dental development over time.
This does not mean every child who mouth breathes will develop facial or dental changes. Growth is influenced by many factors, including genetics, airway anatomy, allergies, dental development, oral habits and general health. It does mean persistent open-mouth breathing, especially during sleep, should be considered in the context of the child’s broader health and development.
In adults, a blocked nose may be associated with poor sleep quality, dry mouth, snoring, morning throat irritation, reduced exercise tolerance or a sense that airflow through the nose is limited. For some patients, the main issue is structural. For others, inflammation from allergy or sinus disease may be more relevant. Many patients have more than one contributing factor.
Dr Simon Braham, ENT and Head and Neck Surgeon at Melbourne ENT, assesses both structure and function. This may include the nasal septum, turbinates, nasal lining, sinus symptoms, tonsils, adenoids in children, and sleep-related concerns where relevant.
What Is Chronic Mouth Breathing?
Mouth breathing means regularly breathing through the mouth instead of the nose. It may happen during the day, during sleep, or both.
Temporary mouth breathing is common. A blocked nose from a cold, a short-term allergy flare, or intense exercise may make mouth breathing necessary for a period of time. This usually improves once the trigger settles.
Chronic mouth breathing is different. It may be noticed as:
- Sleeping with the mouth open
- Waking with a dry mouth
- Snoring
- Noisy breathing at night
- Difficulty keeping the lips closed at rest
- Bad breath or throat dryness
- Tiredness despite enough time in bed
- A blocked or congested nose most days
- A child chewing with the mouth open because nasal breathing seems difficult
Patients often adapt gradually. Adults may not realise how blocked their nose feels until they are specifically asked. Parents may notice that a child sleeps with an open mouth, snores, drools on the pillow, wakes unrefreshed or seems tired and irritable during the day.
Mouth breathing is a symptom pattern, not a diagnosis. The important question is why it is happening.
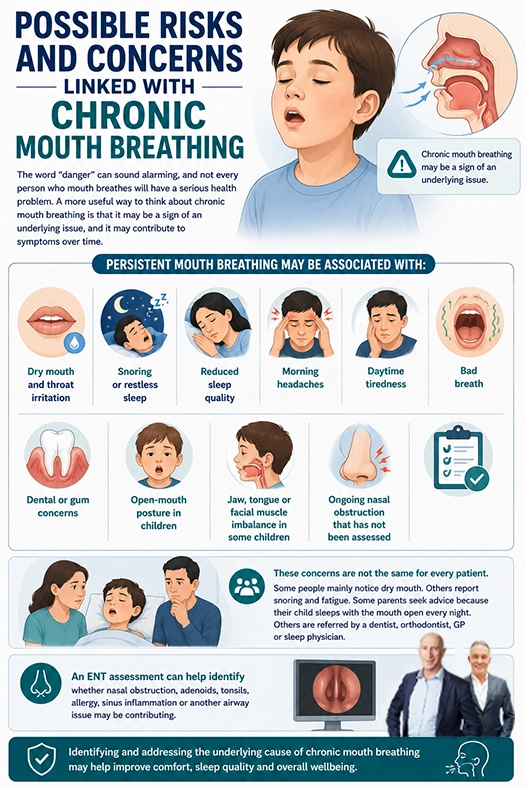
Possible Risks And Concerns Linked With Chronic Mouth Breathing
The word “danger” can sound alarming, and not every person who mouth breathes will have a serious health problem. A more useful way to think about chronic mouth breathing is that it may be a sign of an underlying issue, and it may contribute to symptoms over time.
Persistent mouth breathing may be associated with:
- Dry mouth and throat irritation
- Snoring or restless sleep
- Reduced sleep quality
- Morning headaches
- Daytime tiredness
- Bad breath
- Dental or gum concerns
- Open-mouth posture in children
- Jaw, tongue or facial muscle imbalance in some children
- Ongoing nasal obstruction that has not been assessed
These concerns are not the same for every patient. Some people mainly notice dry mouth. Others report snoring and fatigue. Some parents seek advice because their child sleeps with the mouth open every night. Others are referred by a dentist, orthodontist, GP or sleep physician.
An ENT assessment can help identify whether nasal obstruction, adenoids, tonsils, allergy, sinus inflammation or another airway issue may be contributing.
Common Causes Of Chronic Mouth Breathing
There are several reasons a person may rely on mouth breathing.
✓ Allergic Rhinitis And Hay Fever
Allergic rhinitis is common in Melbourne and across Victoria. Triggers may include pollen, dust mites, mould or pets. Symptoms can include sneezing, an itchy nose, a runny nose, postnasal drip and nasal blockage.
When allergy causes the lining of the nose to swell, airflow may become more difficult. Some people feel blocked on both sides. Others notice that the blockage changes from side to side. Night-time symptoms can be particularly frustrating because lying down may worsen congestion.
For some patients, allergy management may help control symptoms. This may include saline rinses, environmental measures, nasal sprays or other treatments recommended by a doctor. If symptoms are persistent, an ENT assessment may help clarify whether allergy is the main issue or whether structural factors are also contributing.
✓ Enlarged Adenoids In Children
Adenoids are immune tissue located high behind the nose. They are common contributors to nasal obstruction in children. Enlarged adenoids can make it harder for air to pass through the back of the nose, especially during sleep.
A child with enlarged adenoids may snore, breathe through the mouth, have a blocked-sounding nose, develop recurrent nasal discharge, or sleep restlessly. Adenoids can also be relevant in children with recurrent ear problems, depending on the clinical picture.
Assessment is important because not every child with mouth breathing needs surgery. Some children need allergy management, observation or further investigation. Others may benefit from discussion about adenoid or tonsil treatment when symptoms are significant.
✓ Enlarged Tonsils
The tonsils sit at the back of the throat. Enlarged tonsils can narrow the upper airway, particularly during sleep when muscles relax. In children, enlarged tonsils and adenoids are common contributors to sleep-disordered breathing.
Parents may notice snoring, restless sleep, unusual sleeping positions, pauses in breathing, night sweats, bedwetting, daytime tiredness or behavioural changes. These symptoms do not always mean a child has obstructive sleep apnoea, but they should be assessed if they are persistent.
✓ Deviated Septum
The septum is the wall between the left and right sides of the nose. If it is bent or deviated, airflow may be reduced on one or both sides. Some people are born with a deviated septum. Others develop it after an injury.
A deviated septum may be associated with constant blockage, one-sided obstruction, noisy breathing, difficulty exercising through the nose, or worsening congestion during sleep. Septoplasty may be considered when a deviated septum is a significant contributor to symptoms and non-surgical measures have not provided adequate symptom control.
✓ Enlarged Turbinates
Turbinates are normal structures inside the nose. They help warm, humidify and filter air. They can become enlarged due to allergies, irritation, inflammation or natural tissue swelling. Enlarged turbinates may contribute to a blocked nose, especially at night.
Treatment depends on the cause. In some patients, medical management is appropriate. In others, turbinoplasty may be discussed if symptoms persist and the anatomy is suitable.
✓ Chronic Sinus Or Nasal Inflammation
Chronic inflammation in the nose and sinuses may be associated with congestion, facial pressure, postnasal drip, reduced smell, recurrent infections or a heavy blocked feeling. This may contribute to mouth breathing, particularly at night.
Melbourne ENT assesses sinus symptoms alongside the rest of the airway. In some cases, imaging or further investigation may be appropriate.
✓ Habit After Obstruction
Sometimes a person continues to mouth breathe even after the original blockage improves. This can happen in children and adults. In these situations, treatment may involve more than one approach, such as ENT care, dental or orthodontic input, speech therapy, or myofunctional therapy.
Mouth Breathing And Sleep
Mouth breathing and poor sleep often occur together. A blocked nose can make it harder to breathe quietly and comfortably at night. Some people wake frequently because their mouth becomes dry. Others snore or feel unrefreshed despite spending enough time in bed.
Night-time signs that may justify assessment include:
- Regular snoring
- Open-mouth sleeping
- Restless sleep
- Waking with a dry mouth
- Pauses in breathing
- Gasping or choking episodes
- Night sweats in children
- Bedwetting in some children
- Frequent waking
Daytime signs may include:
- Morning headaches
- Tiredness
- Poor concentration
- Irritability
- Behavioural concerns in children
- Reduced exercise tolerance
- Waking unrefreshed
Snoring does not always mean obstructive sleep apnoea. However, persistent snoring, witnessed pauses in breathing, restless sleep or daytime tiredness should be assessed. In children, even when obstructive sleep apnoea is not present, ongoing snoring and poor sleep may still affect daytime function and family wellbeing.
Dr Simon Braham, ENT and Head and Neck Surgeon at Melbourne ENT, commonly assesses patients where nasal obstruction, mouth breathing, snoring and sleep disturbance overlap. Some patients may require a sleep study or referral to a sleep physician, depending on their symptoms and risk factors.
Mouth Breathing And Oral Health
The mouth does not provide the same filtering, warming and humidifying functions as the nose. When a person sleeps with their mouth open, the mouth and throat can become dry. Saliva helps protect the teeth, gums and soft tissues, so a dry mouth may contribute to discomfort and oral health concerns.
Patients may notice:
- Dry mouth on waking
- Bad breath
- Sore throat in the morning
- Cracked lips
- Increased thirst overnight
- Gum irritation
- A coated tongue
- Dental concerns raised by a dentist
ENT care does not replace dental care. If mouth breathing is affecting the teeth, gums or jaw development, a dentist or orthodontist may also be involved. In children, this combined approach may be helpful when airway symptoms and dental development concerns appear together.
Mouth Breathing And Facial Development In Children
Parents often ask whether mouth breathing can affect facial growth. A balanced answer is that persistent mouth breathing may be associated with changes in jaw posture, tongue posture, dental arch development and facial muscle balance, but it is not the only factor.
Children grow in different ways. Genetics, dental development, allergies, tonsil and adenoid size, nasal anatomy, habits and general health all play a role. It would be misleading to say that mouth breathing will always cause facial or dental problems. It would also be unhelpful to ignore persistent symptoms during a child’s growth years.
Possible signs that may justify assessment include:
- Regular open-mouth posture
- Snoring
- Restless sleep
- A blocked nose most days
- Speech or swallowing concerns
- Dental crowding
- A narrow upper jaw
- Difficulty chewing with the mouth closed
- Daytime tiredness or behavioural changes
A child who mouth breathes because of enlarged adenoids, large tonsils, allergy or nasal obstruction may benefit from early review. Treatment is not always surgical. The first step is understanding the cause.
Melbourne ENT sees children from Melbourne and surrounding areas for assessment of nasal obstruction, snoring, tonsil and adenoid concerns, recurrent infections and sleep-related ENT symptoms. Where needed, care may involve the child’s GP, dentist, orthodontist, paediatrician or sleep physician.
Mouth Breathing, Headaches, Jaw Tension And Posture
Some adults and children with chronic mouth breathing also report jaw tension, morning headaches, neck discomfort or facial pressure. These symptoms can have many causes, and it is important not to assume they are all due to the nose.
However, breathing patterns can influence posture. If a person regularly holds the mouth open, drops the jaw forward, or changes head position to breathe more easily, muscle strain may occur. Poor sleep can also contribute to headaches, fatigue and reduced wellbeing.
ENT assessment may be useful when these symptoms occur together with:
- Blocked nasal breathing
- Snoring
- Dry mouth on waking
- Sinus pressure
- Recurrent nasal congestion
- Restless sleep
- Mouth breathing during the day or night
The goal is not to blame every symptom on the nose. The goal is to identify whether nasal obstruction or upper airway narrowing may be contributing to the overall symptom pattern.
What Happens During An ENT Assessment?
A careful ENT assessment begins with the patient’s story. At Melbourne ENT, this includes asking about nasal blockage, allergy symptoms, sinus symptoms, snoring, mouth breathing, sleep quality, recurrent infections, prior nasal injury and previous treatments.
For children, parents may be asked about sleep posture, snoring, pauses in breathing, daytime behaviour, hearing, ear infections, speech, feeding, growth and school concerns. Videos of a child sleeping can sometimes help demonstrate snoring or breathing patterns.
The examination may include assessment of the nose, mouth, tonsils, throat and ears. In selected patients, nasal endoscopy may be recommended. This involves using a small flexible or rigid camera to look inside the nose and, where appropriate, behind the nasal passages. It can help assess the septum, turbinates, nasal lining, mucus, polyps, adenoids and other structures.
If sleep apnoea is suspected, further assessment may be needed. This may involve a sleep study or referral to a sleep physician. The type of investigation depends on the patient’s age, symptoms and medical history.
Dr Simon Braham MBBS (Hons), FRACS, ENT and Head and Neck Surgeon, takes a practical and patient-centred approach. The focus is on explaining what is seen, what it may mean, and what options are reasonable for that particular patient.
Treatment Options For Chronic Mouth Breathing And Nasal Obstruction
Treatment depends on the cause. There is no single treatment that suits every patient.
✓ Medical Treatment For Allergy And Inflammation
When allergy or inflammation is the main issue, treatment may involve saline rinses, allergen reduction, nasal sprays or other medications recommended by a doctor. Some patients may need allergy testing or longer-term allergy management.
Medical treatment is often the first step, especially when the nasal blockage changes with seasons, dust exposure, pets or weather.
✓ Adenoid And Tonsil Treatment
In children with significant snoring, mouth breathing, sleep disturbance or recurrent infections, the adenoids and tonsils may need assessment. If enlarged adenoids or tonsils are contributing to airway obstruction, surgery may be discussed.
This decision depends on the severity of symptoms, examination findings, sleep concerns, age, general health and family preferences. Parents should be given clear information about expected benefits, limitations, risks and recovery.
✓ Septoplasty
Septoplasty is surgery to straighten the nasal septum. It may be considered when a deviated septum is causing significant nasal obstruction. It is usually functional surgery, meaning the aim is to address airflow rather than change the external appearance of the nose.
Some patients also have external nasal concerns or nasal valve issues. In those cases, septoplasty may be discussed as part of a broader surgical plan. The details depend on the patient’s anatomy and goals.
✓ Turbinoplasty
Turbinoplasty is surgery to reduce enlarged turbinates while preserving their important functions as much as possible. It may be considered when turbinate enlargement contributes to persistent nasal blockage and medical treatment has not provided adequate symptom control.
✓ Sinus Treatment
For patients with chronic sinus symptoms, treatment may include medical therapy, imaging, review of contributing factors, or sinus surgery in selected cases. Sinus surgery is not a treatment for every blocked nose, but it may be relevant when chronic sinus disease is present.
✓ Dental, Orthodontic And Allied Health Support
If mouth breathing continues after obstruction is addressed, allied health support may be helpful. This may include dental or orthodontic care, speech therapy or myofunctional therapy in selected patients. This is particularly relevant when tongue posture, oral habits or dental development are part of the picture.
Frequently Asked Questions
Can mouth breathing become a habit even after the blocked nose improves?
Yes. Some people continue to mouth breathe after the original cause has settled, particularly if the pattern has been present for a long time. In these cases, ENT assessment may be combined with dental, orthodontic, speech pathology or myofunctional therapy input.
Why does my child sleep with their mouth open but breathe through the nose during the day?
Nasal blockage can become more noticeable at night because lying down may increase congestion. Enlarged adenoids, enlarged tonsils, allergy or nasal inflammation may also affect night-time breathing more than daytime breathing.
Can a blocked nose affect how refreshed I feel in the morning?
It may contribute, especially if nasal obstruction is associated with snoring, dry mouth, restless sleep or repeated waking. Other sleep, medical and lifestyle factors can also be involved, so assessment is important.
Is mouth taping safe if I have a blocked nose?
Mouth taping is not suitable for everyone and may be unsafe if nasal breathing is restricted or sleep apnoea is suspected. People with persistent mouth breathing should seek medical advice before trying strategies that restrict mouth breathing during sleep.
Can children grow out of mouth breathing?
Some children improve as infections settle or nasal passages grow, but persistent mouth breathing should not be assumed to resolve on its own. Assessment may help identify allergy, enlarged adenoids, tonsil issues or other airway factors.
Why does one side of my nose always feel more blocked than the other?
This may relate to the normal nasal cycle, allergy, turbinate swelling, a deviated septum or other structural factors. If one-sided blockage is persistent or worsening, ENT assessment is appropriate.
Can mouth breathing affect teeth even if there is no pain?
It may contribute to dry mouth, gum irritation or dental development concerns in some patients. A dentist or orthodontist may be involved when mouth breathing occurs alongside bite, palate or tooth alignment concerns.
Why does my nose feel blocked even when there is no mucus?
A blocked feeling can be caused by swelling of the nasal lining, enlarged turbinates, a deviated septum, nasal valve narrowing or inflammation. The nose may feel obstructed even when it is not runny.
Can nasal obstruction and snoring be related without sleep apnoea?
Yes. Nasal obstruction may contribute to snoring or disturbed sleep even when obstructive sleep apnoea is not diagnosed. Persistent snoring, pauses in breathing or daytime tiredness should still be assessed.
Will treating nasal obstruction stop mouth breathing?
It may help in some patients, but results vary depending on the cause and whether mouth breathing has become habitual. Treatment decisions should be based on assessment findings, symptoms and individual circumstances.
Understanding The Cause Is The First Step
Nasal breathing is an important part of normal airway function. The nose filters, warms and humidifies air and contributes to normal upper airway function. When nasal breathing is difficult, some people compensate by breathing through the mouth.
Occasional mouth breathing is common. Persistent mouth breathing, particularly during sleep, may be associated with nasal obstruction, allergy, enlarged adenoids, enlarged tonsils, sinus inflammation or another airway issue. In children, assessment may be helpful when symptoms are ongoing because growth, sleep and breathing patterns can be connected.
At Melbourne ENT, the focus is on careful assessment, clear explanation and individualised care. Not every patient needs surgery. Some patients may benefit from medical treatment, sleep assessment, dental or orthodontic input, or allied health support. Some may be suitable for an ENT procedure when symptoms, anatomy and clinical findings support that option.
To arrange an appointment with Dr Simon Braham MBBS (Hons), FRACS, ENT and Head and Neck Surgeon at Melbourne ENT in St Kilda East, visit the contact us page.
Further Reading
- Read more about Nasal Valve Dysfunction Melbourne
- Read more about Nasal Cautery Surgery
- Read more about Nasal Polyps Surgery (Polypectomy) Melbourne – Also Known as FESS
- Read Melbourne ENT’s Blog on Difficult Breathing? – Understanding Nasal Congestion and Its Causes
- Read Melbourne ENT’s Blog on Allergy Management Tips To Reduce Sinus Flares
- Read Melbourne ENT’s Blog on Common Nose Problems That Nose Surgery May Help